Fill a Valid Ohio Si 7 Form
Fill a Valid Ohio Si 7 Form
Ohio Department of Taxation Forms - It is crucial for applicants to ensure all sections of the RCB 020 are completed before submission.
For those looking to create or learn more about the Georgia Quitclaim Deed form, resources can be found at smarttemplates.net, where you can find templates and guidance for effectively transferring property ownership while understanding the limitations of this legal document.
Vender License Ohio - Form ST 1T is regularly updated; check for the latest version before submission.
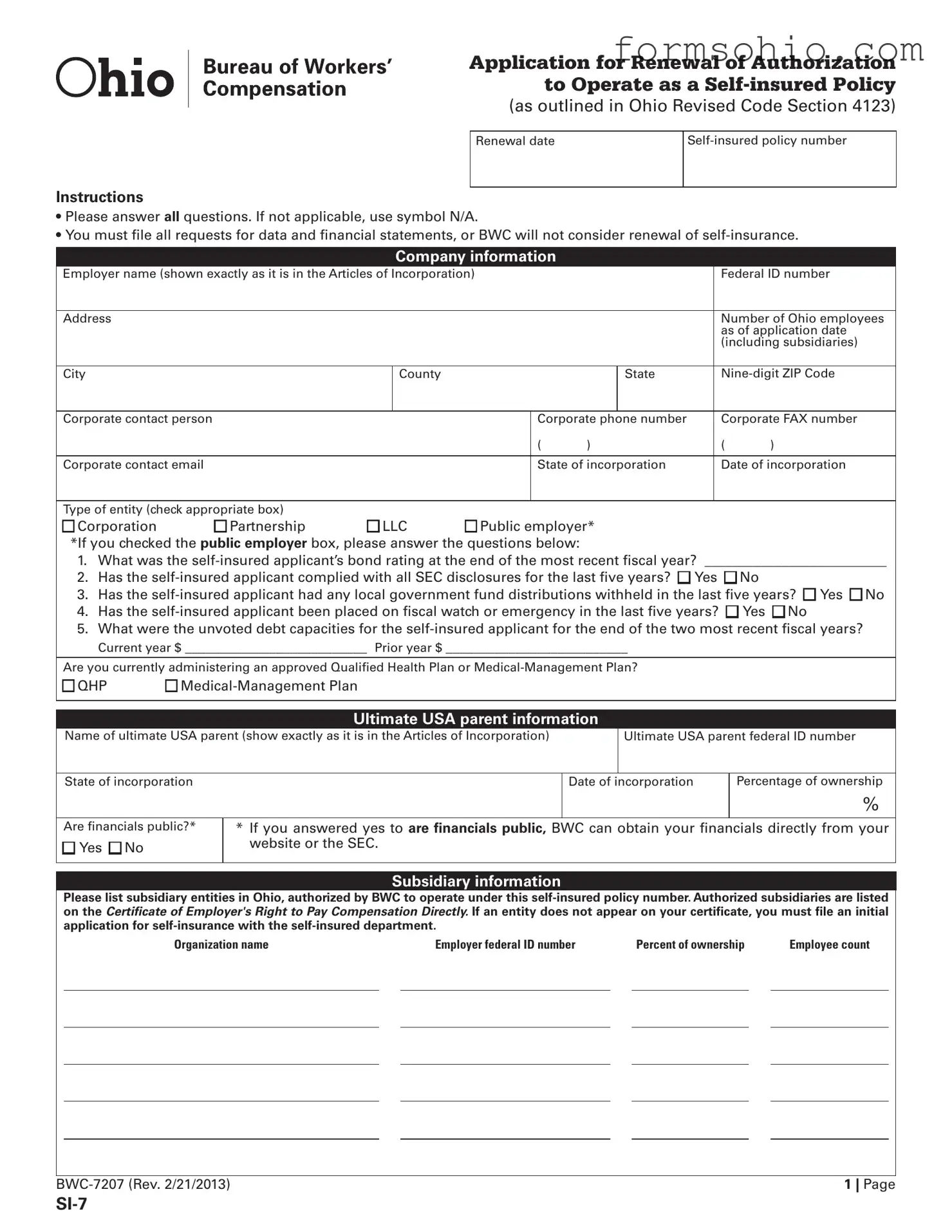
Application for Renewal of Authorization to Operate as a
(as outlined in Ohio Revised Code Section 4123)
Renewal date
Instructions
•Please answer all questions. If not applicable, use symbol N/A.
•You must ile all requests for data and inancial statements, or BWC will not consider renewal of
Company information
Employer name (shown exactly as it is in the Articles of Incorporation) |
|
|
|
Federal ID number |
|||||||
|
|
|
|
|
|
|
|
|
|
||
Address |
|
|
|
|
|
|
|
|
Number of Ohio employees |
||
|
|
|
|
|
|
|
|
|
|
as of application date |
|
|
|
|
|
|
|
|
|
|
|
(including subsidiaries) |
|
|
|
|
|
|
|
|
|
|
|
|
|
City |
|
|
|
County |
|
|
|
State |
|
||
|
|
|
|
|
|
|
|
|
|||
Corporate contact person |
|
|
|
|
Corporate phone number |
|
Corporate FAX number |
||||
|
|
|
|
|
|
( |
) |
|
|
( |
) |
|
|
|
|
|
|
|
|
|
|||
Corporate contact email |
|
|
|
|
State of incorporation |
|
Date of incorporation |
||||
|
|
|
|
|
|
|
|
|
|
||
Type of entity (check appropriate box) |
|
|
|
|
|
|
|
|
|
||
n Corporation |
n Partnership |
n LLC |
n Public employer* |
|
|
||||||
*If you checked the public employer box, please answer the questions below: |
|
|
|
|
|
||||||
1. |
What was the |
||||||||||
2. |
Has the |
|
n No |
||||||||
3. |
Has the |
||||||||||
4. |
Has the |
||||||||||
5. What were the unvoted debt capacities for the
Are you currently administering an approved Qualiied Health Plan or
n QHP |
n |
Ultimate USA parent information
Name of ultimate USA parent (show exactly as it is in the Articles of Incorporation) |
|
Ultimate USA parent federal ID number |
||
|
|
|
|
|
State of incorporation |
|
Date of incorporation |
Percentage of ownership |
|
|
|
|
|
% |
|
|
|
|
|
Are inancials public?* |
* If you answered yes to are financials public, BWC can obtain your inancials directly from your |
|||
n Yes n No |
website or the SEC. |
|
|
|
|
|
|
|
|
|
|
|
|
|
Subsidiary information
Please list subsidiary entities in Ohio, authorized by BWC to operate under this
Organization name |
|
Employer federal ID number |
|
Percent of ownership |
|
Employee count |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1 | Page |

Subsidiary information
|
Organization name |
|
Employer federal ID number |
|
Percent of ownership |
Employee count |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2 | Page |
Corporate restructuring
Please note: For BWC to properly process the referenced revisions, please provide Ohio secretary of state papers and updated organizational chart.
Has your corporate name, structure or ultimate U.S. parent changed during the past year?
n Yes n No
If yes, please provide detailed explanation: ____________________________________________________________________________________________
Ohio administrator information
Note:This administrator must be an employee of your company. It cannot be yourTPA.
Has your Ohio administrator changed in the last 12 months? n Yes n No
Does the Ohio administrator have one or more years of experience as a workers' compensation administrator for
Ohio administrator's name
Ohio administrator’s fax number
( )
Ohio administrator’s email address
Authorized representative
Has the authorized representative changed in the last 12 months? n Yes n No
Representative name
Representative identiication number |
Representative phone number |
|
|
( |
) |
Email address |
|
|
Excess workers' compensation insurance
Does your company carry excess workers' compensation insurance?* n Yes n No
*If you answered yes to does your company carry excess workers' compensation insurance, please submit a copy of the policies declaration page to SIINQ@bwc.state.oh.us
Name of carrier: _____________________________________________________________________________________________________________________
Name of agent: ______________________________________________________Telephone number: (________)____________________________________
Policy number: _______________________________________________________________________________________________________________________
Current policy period: From ______________________________________ to _________________________________________________________________
Is excess insurance paying claims?*
n Yes n No *If yes, please submit claim number(s) on a separate document to siinq@bwc.state.oh.us
Ohio assets and gross payroll information
Calendar and/or iscal year ending __________/__________/__________
MM DD YYYY
Ohio assets: $ ____________________________________________________
Ohio gross payroll: $ ______________________________________________
|
|
Certification |
|||
|
(Notary seal) |
|
|
|
|
|
State of ______________________ County of _________________________ ss _______________________________ being duly sworn says that he/she |
||||
|
is the ____________________________ of ____________________________ , the employer referred to in the foregoing is true to the best of their knowledge. |
||||
|
Sworn to before me, this ________ day of ______________________ , 20_______ . |
||||
|
|
|
|
|
|
|
Notary signature |
|
Corporate oficer signature |
||
|
|
|
|
|
|
|
|
3 | Page |
|||

|
Claim File Housing Locations |
Instructions |
|
• Indicate all locations where you maintain claims records for auditing |
Company: ______________________________________ |
purposes (including authorized reps). |
This form completed by
Name and title
Telephone number
( )
Company/authorized representative: _________________________________________________________________________
Contact name: ______________________________________________________________________________________________
Telephone number: __________________________________________________________________________________________
Address: ____________________________________________________________________________________________________
_____________________________________________________________________________________________________________
Email address: _________________________________________________________________________________________________
Date range of claims: _________________________________________________________________________________________
Approximate number of claims housed in this location? _______________________________________________________
Company/authorized representative: _________________________________________________________________________
Contact name: ______________________________________________________________________________________________
Telephone number: __________________________________________________________________________________________
Address: ____________________________________________________________________________________________________
_____________________________________________________________________________________________________________
Email address: _________________________________________________________________________________________________
Date range of claims: _________________________________________________________________________________________
Approximate number of claims housed in this location? _______________________________________________________
Company/authorized representative: _________________________________________________________________________
Contact name: ______________________________________________________________________________________________
Telephone number: __________________________________________________________________________________________
Address: ____________________________________________________________________________________________________
_____________________________________________________________________________________________________________
Email address: _________________________________________________________________________________________________
Date range of claims: _________________________________________________________________________________________
Approximate number of claims housed in this location? _______________________________________________________
4 | Page |

Company/authorized representative: _________________________________________________________________________
Contact name: ______________________________________________________________________________________________
Telephone number: __________________________________________________________________________________________
Address: ____________________________________________________________________________________________________
_____________________________________________________________________________________________________________
Email address: _________________________________________________________________________________________________
Date range of claims: _________________________________________________________________________________________
Approximate number of claims housed in this location? _______________________________________________________
Company/authorized representative: _________________________________________________________________________
Contact name: ______________________________________________________________________________________________
Telephone number: __________________________________________________________________________________________
Address: ____________________________________________________________________________________________________
_____________________________________________________________________________________________________________
Email address: _________________________________________________________________________________________________
Date range of claims: _________________________________________________________________________________________
Approximate number of claims housed in this location? _______________________________________________________
Company/authorized representative: _________________________________________________________________________
Contact name: ______________________________________________________________________________________________
Telephone number: __________________________________________________________________________________________
Address: ____________________________________________________________________________________________________
_____________________________________________________________________________________________________________
Email address: _________________________________________________________________________________________________
Date range of claims: _________________________________________________________________________________________
Approximate number of claims housed in this location? _______________________________________________________
Company/authorized representative: _________________________________________________________________________
Contact name: ______________________________________________________________________________________________
Telephone number: __________________________________________________________________________________________
Address: ____________________________________________________________________________________________________
_____________________________________________________________________________________________________________
Email address: _________________________________________________________________________________________________
Date range of claims: _________________________________________________________________________________________
Approximate number of claims housed in this location? _______________________________________________________
5 | Page |

Company/authorized representative: _________________________________________________________________________
Contact name: ______________________________________________________________________________________________
Telephone number: __________________________________________________________________________________________
Address: ____________________________________________________________________________________________________
_____________________________________________________________________________________________________________
Email address: _________________________________________________________________________________________________
Date range of claims: _________________________________________________________________________________________
Approximate number of claims housed in this location? _______________________________________________________
Company/authorized representative: _________________________________________________________________________
Contact name: ______________________________________________________________________________________________
Telephone number: __________________________________________________________________________________________
Address: ____________________________________________________________________________________________________
_____________________________________________________________________________________________________________
Email address: _________________________________________________________________________________________________
Date range of claims: _________________________________________________________________________________________
Approximate number of claims housed in this location? _______________________________________________________
Company/authorized representative: _________________________________________________________________________
Contact name: ______________________________________________________________________________________________
Telephone number: __________________________________________________________________________________________
Address: ____________________________________________________________________________________________________
_____________________________________________________________________________________________________________
Email address: _________________________________________________________________________________________________
Date range of claims: _________________________________________________________________________________________
Approximate number of claims housed in this location? _______________________________________________________
Company/authorized representative: _________________________________________________________________________
Contact name: ______________________________________________________________________________________________
Telephone number: __________________________________________________________________________________________
Address: ____________________________________________________________________________________________________
_____________________________________________________________________________________________________________
Email address: _________________________________________________________________________________________________
Date range of claims: _________________________________________________________________________________________
Approximate number of claims housed in this location? _______________________________________________________
6 | Page |
|
Subsidiary Update Request |
Instructions |
|
• List all approved subsidiary entities, including address, |
|
contact, phone and email information. |
Company: _________________________________________ |
This form completed by
Name and title
Telephone number
( )
|
|
Subsidiary name: _________________________________________ |
|
|
Attention:_________________________________________________ |
|
|
Telephone number: _______________________________________ |
|
|
Address:__________________________________________________ |
The existing subsidiary has been |
|
|
Closed |
Sold |
__________________________________________________________ |
Check if there are no changes |
Email address: ____________________________________________ |
|
|
|
|
|
|
Subsidiary name: _________________________________________ |
|
|
Attention:_________________________________________________ |
|
|
Telephone number: _______________________________________ |
|
|
Address:__________________________________________________ |
The existing subsidiary has been |
|
|
Closed |
Sold |
__________________________________________________________ |
Check if there are no changes |
Email address: ____________________________________________ |
|
|
|
|
|
|
Subsidiary name: _________________________________________ |
|
|
Attention:_________________________________________________ |
|
|
Telephone number: _______________________________________ |
|
|
Address:__________________________________________________ |
The existing subsidiary has been |
|
|
Closed |
Sold |
__________________________________________________________ |
Check if there are no changes |
Email address: ____________________________________________ |
|
|
|
|
7 | Page |
|
|
Subsidiary name: _________________________________________ |
|
|
Attention:_________________________________________________ |
|
|
Telephone number: _______________________________________ |
|
|
Address:__________________________________________________ |
The existing subsidiary has been |
|
|
Closed |
Sold |
__________________________________________________________ |
Check if there are no changes |
Email address: ____________________________________________ |
|
|
|
|
|
|
Subsidiary name: _________________________________________ |
|
|
Attention:_________________________________________________ |
|
|
Telephone number: _______________________________________ |
|
|
Address:__________________________________________________ |
The existing subsidiary has been |
|
|
Closed |
Sold |
__________________________________________________________ |
Check if there are no changes |
Email address: ____________________________________________ |
|
|
|
|
|
|
Subsidiary name: _________________________________________ |
|
|
Attention:_________________________________________________ |
|
|
Telephone number: _______________________________________ |
|
|
Address:__________________________________________________ |
The existing subsidiary has been |
|
|
Closed |
Sold |
__________________________________________________________ |
Check if there are no changes |
Email address: ____________________________________________ |
|
|
|
|
|
|
Subsidiary name: _________________________________________ |
|
|
Attention:_________________________________________________ |
|
|
Telephone number: _______________________________________ |
|
|
Address:__________________________________________________ |
The existing subsidiary has been |
|
|
Closed |
Sold |
__________________________________________________________ |
Check if there are no changes |
Email address: ____________________________________________ |
|
|
|
|
8 | Page |
| Fact Name | Description |
|---|---|
| Purpose | The Ohio SI 7 form is used to apply for the renewal of authorization to operate as a self-insured policy under Ohio law. |
| Governing Law | This form is governed by the Ohio Revised Code Section 4123, which outlines the regulations for self-insured employers. |
| Submission Requirements | Applicants must answer all questions on the form. If a question is not applicable, they should indicate this by using "N/A". |
| Financial Disclosure | Failure to file requests for data and financial statements may result in the denial of the renewal for self-insurance. |
The Ohio SI 7 form is an important document for companies seeking to renew their authorization to operate as self-insured employers. Along with this form, several other documents may be required to ensure compliance with state regulations. Below is a list of additional forms that are commonly used in conjunction with the Ohio SI 7 form.
Gathering these documents alongside the Ohio SI 7 form can help streamline the renewal process and ensure compliance with state requirements. It is advisable to review all requirements carefully to avoid delays.
Completing the Ohio SI 7 form is essential for employers seeking to renew their authorization to operate as a self-insured entity. It requires detailed information about the company, its structure, and its financial status. Following these steps will help ensure the form is filled out accurately and completely.
Completing the Ohio SI-7 form accurately is crucial for maintaining self-insured status. One common mistake is failing to answer all questions. Each section of the form must be addressed. If a question does not apply, it is important to indicate this by using "N/A." Omitting this can lead to delays in processing.
Another frequent error involves incorrect or incomplete company information. Employers should ensure that the name is entered exactly as it appears in the Articles of Incorporation. Inaccurate federal ID numbers or addresses can complicate the review process. Additionally, providing the wrong number of Ohio employees as of the application date can lead to significant issues.
Many applicants neglect to update their corporate contact details. It is essential to provide the current corporate contact person's name, phone number, and email address. Outdated information can hinder communication and lead to misunderstandings.
Some applicants overlook the requirement to submit financial statements and data requests. Without these documents, the Bureau of Workers' Compensation (BWC) will not consider the renewal. This oversight can result in the denial of the self-insured application.
Additionally, not providing accurate subsidiary information is a common mistake. Employers must list all subsidiary entities authorized by the BWC to operate under the self-insured policy number. Failing to do so can result in complications regarding coverage and compliance.
Another mistake involves the failure to disclose changes in corporate structure or ownership. If there have been changes within the past year, a detailed explanation must be provided. Neglecting this requirement can raise red flags during the review process.
Some applicants do not verify the experience of their Ohio administrator. The administrator must be an employee of the company and should have at least one year of experience as a workers' compensation administrator for self-insured employers in Ohio. This information is critical for ensuring proper administration of claims.
It is also important to accurately report on excess workers' compensation insurance. If the company carries this insurance, a copy of the policy's declaration page must be submitted. Failure to provide this documentation can lead to questions about coverage.
Lastly, applicants sometimes forget to certify the form properly. The certification must be signed by an authorized corporate officer, and the notary seal must be included. Incomplete certification can delay the processing of the application.
What is the Ohio SI 7 form?
The Ohio SI 7 form is the Application for Renewal of Authorization to Operate as a Self-insured Policy. It is a required document for employers seeking to continue their self-insured status under Ohio Revised Code Section 4123. Completing this form accurately is essential for maintaining compliance and ensuring uninterrupted self-insured coverage.
Who needs to fill out the SI 7 form?
Employers who currently hold a self-insured policy in Ohio must complete the SI 7 form to renew their authorization. This includes corporations, partnerships, LLCs, and public employers. Accurate information about the company's operations, financial status, and compliance history is necessary for the renewal process.
What information is required on the form?
The form requires detailed company information, including:
Public employers must provide additional information regarding bond ratings and compliance with SEC disclosures.
What happens if I do not submit all required information?
If you fail to provide all necessary information or financial statements, the Bureau of Workers' Compensation (BWC) will not consider your renewal application. It is crucial to ensure that all sections are completed and any required documents are attached to avoid delays or denial of your renewal.
Can I submit the SI 7 form electronically?
Yes, the SI 7 form can be submitted electronically. Ensure that you follow the specific instructions provided by the BWC for electronic submissions. It is important to keep a copy of the submitted form for your records.
What if my corporate structure has changed?
If your corporate name, structure, or ultimate U.S. parent has changed in the past year, you must provide a detailed explanation in the designated section of the form. Additionally, you should include any relevant documentation, such as Ohio Secretary of State papers and an updated organizational chart.
Is there a deadline for submitting the SI 7 form?
Yes, there is a deadline for submitting the SI 7 form. It is essential to check the specific renewal date for your self-insured policy and submit your application well in advance. Late submissions may result in a lapse in your self-insured coverage.
What should I do if I have questions while filling out the form?
If you have questions while completing the SI 7 form, it is advisable to contact the BWC directly. They can provide guidance and clarify any uncertainties you may have regarding the application process.
What are the consequences of failing to renew my self-insured policy?
Failing to renew your self-insured policy can lead to significant consequences, including the loss of self-insured status. This may result in increased costs and legal liabilities, as you would then be required to obtain traditional workers' compensation insurance coverage.