Fill a Valid Ohio Rcb 020 Form
Fill a Valid Ohio Rcb 020 Form
Odrc Visiting Form - The form requires the visitor's relationship to the inmate, whether friend or relative.
When considering the implications of the California Power of Attorney form, it is crucial to understand not only its structure but also the resources available for obtaining it. Individuals looking to create this important legal document can find reliable templates and information at documentonline.org/blank-california-power-of-attorney, ensuring that their decisions are properly documented and respected.
Ohio Tax Forms - Completing the form accurately can ease future audits and reviews.
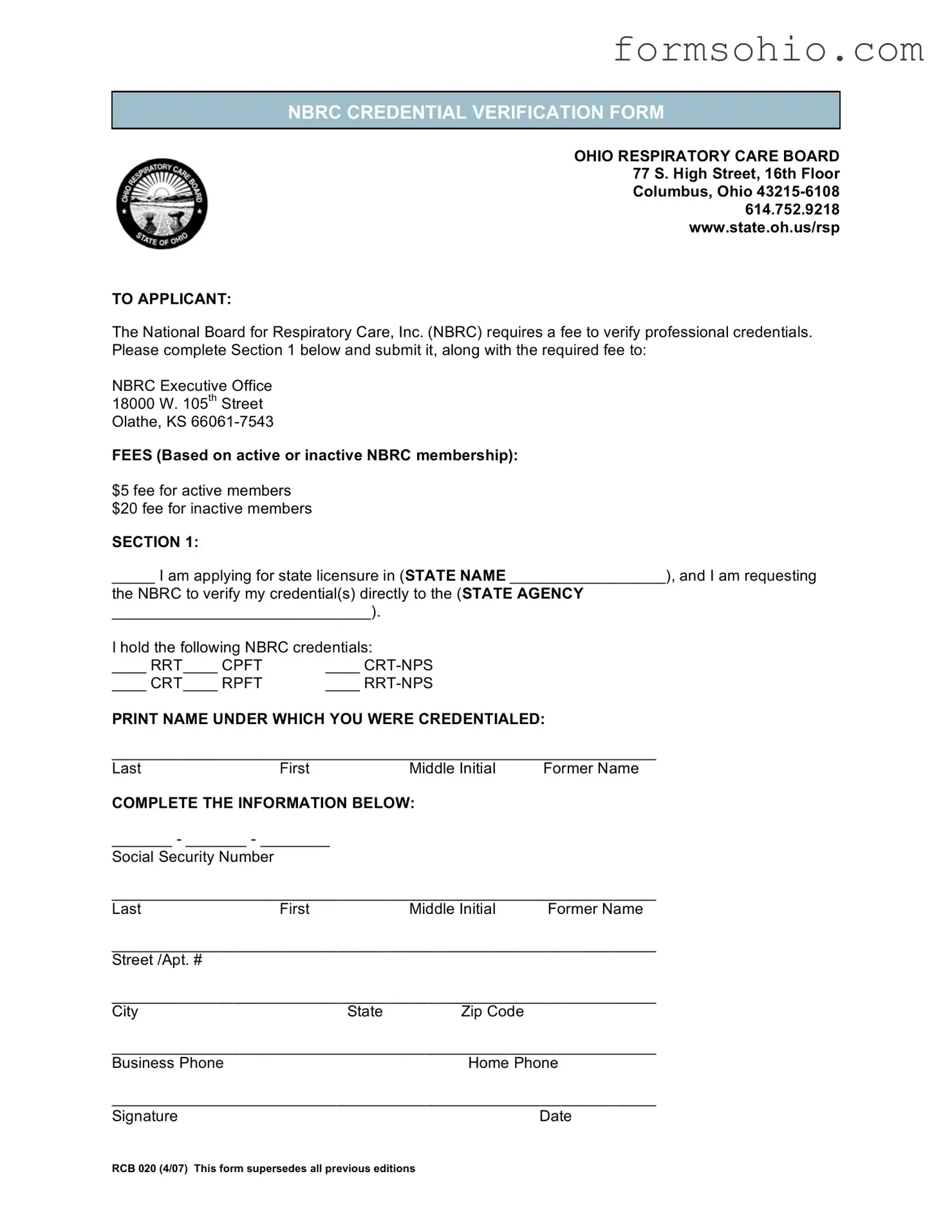
NBRC CREDENTIAL VERIFICATION FORM
OHIO RESPIRATORY CARE BOARD 77 S. High Street, 16th Floor Columbus, Ohio
TO APPLICANT:
The National Board for Respiratory Care, Inc. (NBRC) requires a fee to verify professional credentials. Please complete Section 1 below and submit it, along with the required fee to:
NBRC Executive Office
18000 W. 105th Street
Olathe, KS
FEES (Based on active or inactive NBRC membership):
$5 fee for active members $20 fee for inactive members
SECTION 1:
_____ I am applying for state licensure in (STATE NAME __________________), and I am requesting
the NBRC to verify my credential(s) directly to the (STATE AGENCY
______________________________).
I hold the following NBRC credentials:
____ RRT____ CPFT |
____ |
____ CRT____ RPFT |
____ |
PRINT NAME UNDER WHICH YOU WERE CREDENTIALED:
_______________________________________________________________
Last |
First |
Middle Initial |
Former Name |
COMPLETE THE INFORMATION BELOW: |
|
||
_______ - _______ - ________
Social Security Number
_______________________________________________________________
LastFirst Middle Initial Former Name
_______________________________________________________________
Street /Apt. #
_______________________________________________________________
CityState Zip Code
_______________________________________________________________
Business PhoneHome Phone
_______________________________________________________________
Signature |
Date |
RCB 020 (4/07) This form supersedes all previous editions |
|
| Fact Name | Details |
|---|---|
| Form Title | Ohio RCB 020 is officially known as the NBRC Credential Verification Form. |
| Governing Body | This form is governed by the Ohio Respiratory Care Board. |
| Submission Address | Applicants must submit the form to the NBRC Executive Office in Olathe, Kansas. |
| Verification Fee | The fee for verifying credentials is $5 for active NBRC members and $20 for inactive members. |
| Purpose | The form is used to request verification of professional credentials for state licensure. |
| Required Information | Applicants need to provide personal information including name, social security number, and contact details. |
| Credential Types | Various NBRC credentials can be verified, including RRT, CPFT, CRT-NPS, CRT, RPFT, and RRT-NPS. |
| Signature Requirement | Applicants must sign and date the form to validate their request. |
| Edition Superseded | This edition of the form supersedes all previous versions. |
When applying for licensure in Ohio, several forms and documents accompany the Ohio RCB 020 form. Each of these documents plays a crucial role in ensuring that your application is complete and that your credentials are verified appropriately. Below is a list of commonly used forms that you may need to consider.
Each of these forms contributes to a thorough review of your qualifications and ensures that the licensing process proceeds smoothly. It’s important to gather all necessary documents to avoid delays in your application. Being organized and prepared will help you navigate the process with confidence.
Completing the Ohio RCB 020 form is an essential step in the credential verification process. This form must be filled out accurately to ensure that your professional credentials are verified by the National Board for Respiratory Care (NBRC). Follow these steps carefully to complete the form.
When filling out the Ohio RCB 020 form, one common mistake is neglecting to provide the correct state name where you are applying for licensure. This section is crucial, as it ensures that your credentials are sent to the appropriate state agency. Without this information, the verification process may be delayed or even halted.
Another frequent error involves the Social Security Number section. Applicants sometimes enter their number incorrectly, which can lead to significant issues. A simple typo can cause problems in verifying your identity and credentials. Make sure to double-check the numbers you provide to avoid unnecessary complications.
Many individuals also forget to include their signature and date at the bottom of the form. This step is essential for validating your application. Without a signature, the form may be considered incomplete, leading to further delays in processing your request.
Finally, applicants often overlook the required fee based on their NBRC membership status. It is important to include the correct payment amount to avoid delays in processing. Remember, active members pay $5, while inactive members owe $20. Failing to include the correct fee can result in your application being returned.
The Ohio RCB 020 form is a credential verification form required by the Ohio Respiratory Care Board. It is used to verify professional credentials for individuals applying for state licensure in respiratory care.
Individuals applying for state licensure in Ohio and who hold credentials from the National Board for Respiratory Care (NBRC) must complete this form. This includes those with active or inactive NBRC memberships.
You will need to provide your personal information, including your name, Social Security number, contact details, and the specific NBRC credentials you hold. Additionally, you must indicate the state agency to which you want your credentials verified.
There is a fee required for the verification of credentials. If you are an active NBRC member, the fee is $5. For inactive members, the fee is $20. Payment must be submitted along with the completed form.
After completing the form, send it along with the required fee to the NBRC Executive Office at:
18000 W. 105th Street
Olathe, KS 66061-7543
You can request verification for several NBRC credentials, including:
Yes, you must include your Social Security number on the form. This information is necessary for the verification process.
If you have a former name, you should provide that information on the form. This helps ensure accurate verification of your credentials.
You can contact the Ohio Respiratory Care Board at the following phone number: 614.752.9218. They can assist you with any questions regarding the form or the licensure process.