Fill a Valid Ohio Os 24 Form
Fill a Valid Ohio Os 24 Form
Free Cdl Training Ohio - Applicants need to report any past accidents and their involvement in them.
Ohio Cat Annual Minimum Tax - Communicate with your tax representative throughout the process.
Felony 2 Sentencing in Ohio - Falsification of information on the application can lead to denial of the permit.
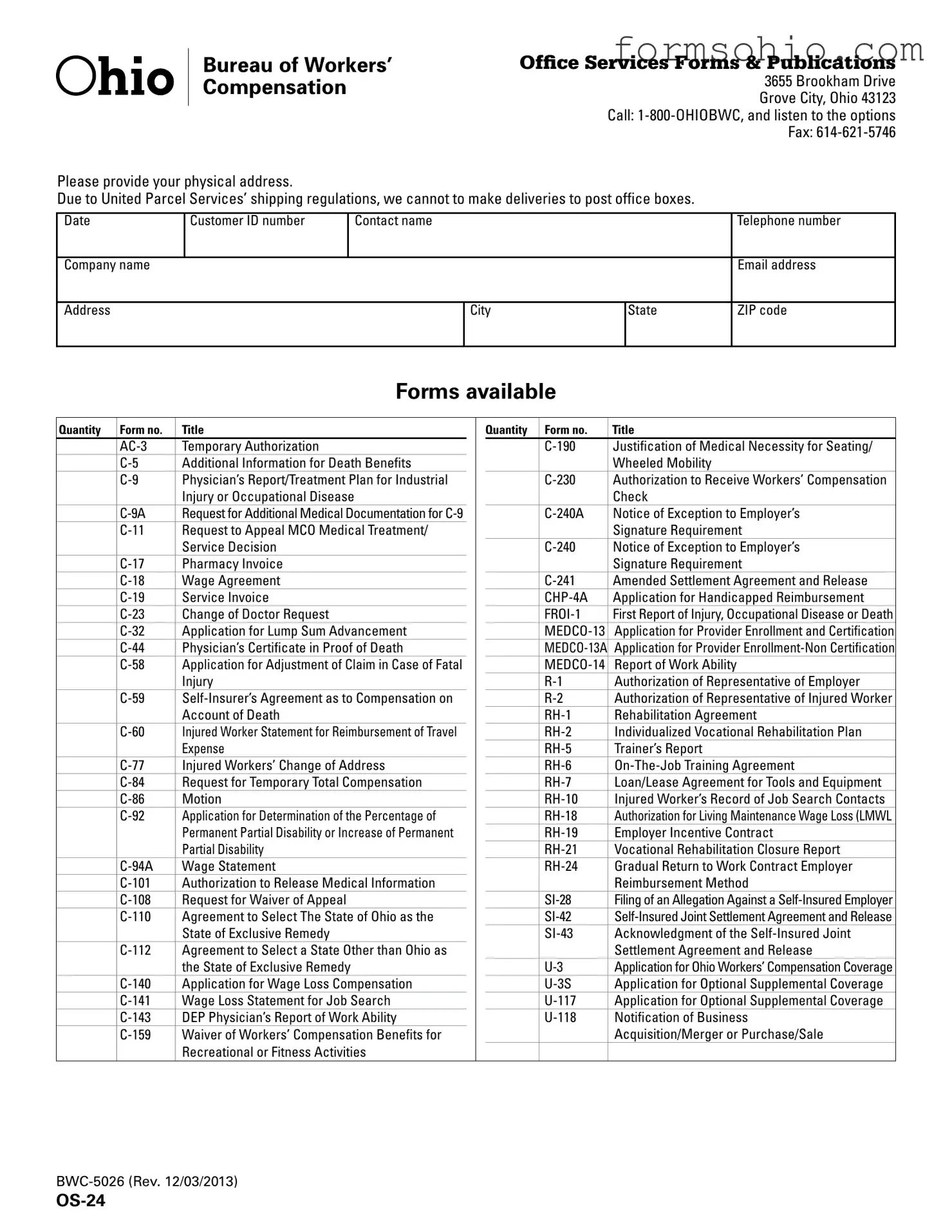
OFfiCE SERVICES FORMS & PUBLICATIONS 3655 Brookham Drive Grove City, Ohio 43123
Call:
Please provide your physical address.
Due to United Parcel Services’ shipping regulations, we cannot to make deliveries to post office boxes.
Date |
Customer ID number |
Contact name |
|
|
Telephone number |
|
|
|
|
|
|
Company name |
|
|
|
|
Email address |
|
|
|
|
|
|
Address |
|
|
City |
State |
ZIP code |
|
|
|
|
|
|
FORMS AVAILABLE
Quantity Form no. |
Title |
Temporary Authorization |
|
Additional Information for Death Benefits |
|
Physician’s Report/Treatment Plan for Industrial |
|
|
Injury or Occupational Disease |
Request for Additional Medical Documentation for |
|
Request to Appeal MCO Medical Treatment/ |
|
|
Service Decision |
Pharmacy Invoice |
|
Wage Agreement |
|
Service Invoice |
|
Change of Doctor Request |
|
Application for Lump Sum Advancement |
|
Physician’s Certificate in Proof of Death |
|
Application for Adjustment of Claim in Case of Fatal |
|
|
Injury |
|
Account of Death |
Injured Worker Statement for Reimbursement of Travel |
|
|
Expense |
Injured Workers’ Change of Address |
|
Request for Temporary Total Compensation |
|
Motion |
|
Application for Determination of the Percentage of |
|
|
Permanent Partial Disability or Increase of Permanent |
|
Partial Disability |
Wage Statement |
|
Authorization to Release Medical Information |
|
Request for Waiver of Appeal |
|
Agreement to Select The State of Ohio as the |
|
|
State of Exclusive Remedy |
Agreement to Select a State Other than Ohio as |
|
|
the State of Exclusive Remedy |
Application for Wage Loss Compensation |
|
Wage Loss Statement for Job Search |
|
DEP Physician’s Report of Work Ability |
|
Waiver of Workers’ Compensation Benefits for |
|
|
Recreational or Fitness Activities |
Quantity |
Form no. |
Title |
|
Justification of Medical Necessity for Seating/ |
|
|
|
Wheeled Mobility |
|
Authorization to Receive Workers’ Compensation |
|
|
|
Check |
|
Notice of Exception to Employer’s |
|
|
|
Signature Requirement |
|
Notice of Exception to Employer’s |
|
|
|
Signature Requirement |
|
Amended Settlement Agreement and Release |
|
|
Application for Handicapped Reimbursement |
|
|
First Report of Injury, Occupational Disease or Death |
|
|
Application for Provider Enrollment and Certification |
|
|
Application for Provider |
|
|
Report of Work Ability |
|
|
Authorization of Representative of Employer |
|
|
Authorization of Representative of Injured Worker |
|
|
Rehabilitation Agreement |
|
|
Individualized Vocational Rehabilitation Plan |
|
|
Trainer’s Report |
|
|
||
|
Loan/Lease Agreement for Tools and Equipment |
|
|
Injured Worker’s Record of Job Search Contacts |
|
|
Authorization for Living Maintenance Wage Loss (LMWL |
|
|
Employer Incentive Contract |
|
|
Vocational Rehabilitation Closure Report |
|
|
Gradual Return to Work Contract Employer |
|
|
|
Reimbursement Method |
|
Filing of an Allegation Against a |
|
|
||
|
Acknowledgment of the |
|
|
|
Settlement Agreement and Release |
|
Application for Ohio Workers’ Compensation Coverage |
|
|
Application for Optional Supplemental Coverage |
|
|
Application for Optional Supplemental Coverage |
|
|
Notification of Business |
|
|
|
Acquisition/Merger or Purchase/Sale |
|
|
|
PUBLICATIONS AVAILABLE
Quantity |
Form number |
Title |
|
CD 106 |
BWC Medical Guide |
|
FB |
Fraud Brochure |
|
FBLW |
Fraud Brochure Law |
|
FBMCO |
Fraud Brochure MCO |
|
FBSI |
Fraud Brochure Self Insured |
|
FFFI |
Fraud Flyer Financial |
Quantity |
Form number |
Title |
|
FFPH |
Fraud Flyer Pharmacy |
|
FP 01 |
Fraud Poster |
|
FS 01 |
Fraud Sticker |
|
FS 01 |
Fraud Sticker |
|
Forms & Publications List |
|
|
PERRP |
Safety and Health Protection on the Job Poster |
Prepared by
Agent number |
Initials |
|
|
Forms that are not listed here are not available through BWC office services forms and publications.
You may obtain Industrial Commission of Ohio (IC) forms by calling the IC forms and
publications number at
| Fact Name | Fact Description |
|---|---|
| Form Purpose | The Ohio OS-24 form is used to request various forms and publications related to workers' compensation. |
| Governing Law | This form is governed by Ohio Revised Code Chapter 4123, which outlines the state's workers' compensation laws. |
| Physical Address Requirement | Applicants must provide a physical address for delivery, as post office boxes are not accepted. |
| Contact Information | Users must include their customer ID, name, telephone number, company name, email address, and full address. |
| Available Forms | The OS-24 form lists numerous available forms, such as the AC-3 Temporary Authorization and C-5 Additional Information for Death Benefits. |
| Submission Methods | Forms can be submitted via fax or phone. The fax number is 614-621-5746, and assistance is available by calling 1-800-OHIOBWC. |
| Updates | The OS-24 form was last revised on December 3, 2013, indicating the need to check for updates periodically. |
The Ohio OS-24 form is a vital document used in various workers' compensation processes. Alongside this form, several other documents may be necessary to support claims, provide additional information, or facilitate communication between parties. Below is a list of forms and documents commonly used in conjunction with the Ohio OS-24 form, each with a brief description to clarify its purpose.
These documents are essential for ensuring that all necessary information is provided and that claims are processed efficiently. It is crucial to have the correct forms completed and submitted in a timely manner to avoid delays in benefits or services. Always consult with a professional if you have questions about any specific form or its requirements.
After completing the Ohio OS-24 form, you will submit it to the appropriate office to request the forms and publications you need. Ensure all information is accurate to avoid delays.
When filling out the Ohio OS-24 form, individuals often make several common mistakes that can lead to delays or complications in processing their requests. One frequent error is providing an incorrect or incomplete physical address. It is essential to remember that deliveries cannot be made to post office boxes due to shipping regulations. Ensuring that the physical address is accurate and complete, including the city, state, and ZIP code, is crucial for timely processing.
Another mistake occurs when applicants fail to include necessary contact information. The form requires a contact name and telephone number, yet many individuals overlook this requirement. Without this information, the processing office may have difficulty reaching out for clarification or additional information, which can slow down the entire process.
Additionally, people sometimes neglect to check the quantity of forms they need. The OS-24 form allows users to request multiple forms, but if the quantity is left blank or inaccurately filled out, it can result in receiving fewer forms than needed. This oversight can lead to frustration and additional time spent re-submitting requests.
Some individuals also make the mistake of not reviewing the specific form numbers and titles before submission. Each form has a designated number that corresponds to its purpose. Failing to select the correct form number can lead to receiving the wrong documentation, which may not meet the applicant's needs.
Moreover, applicants often forget to sign the form. A signature is a critical component of the OS-24 form, as it verifies that the information provided is accurate and complete. Submitting the form without a signature can result in immediate rejection, causing delays in processing.
Lastly, individuals may overlook the importance of checking for any updates or changes to the form requirements. Regulations and forms can change, and it is vital to ensure that the most current version of the OS-24 form is being used. Using outdated forms can lead to confusion and potential issues with processing requests.
The Ohio OS-24 form is a comprehensive list of available forms and publications related to workers' compensation in Ohio. It serves as a resource for individuals and businesses needing specific documentation for claims, appeals, and other related processes.
You can obtain the Ohio OS-24 form by contacting the Office of Workers' Compensation. The office is located at 3655 Brookham Drive, Grove City, Ohio 43123. You can also call 1-800-OHIOBWC for assistance or send a fax to 614-621-5746. Please ensure that you provide a physical address, as deliveries cannot be made to post office boxes.
The OS-24 includes a variety of forms designed for different purposes. For instance, it lists forms for temporary authorizations, medical documentation requests, appeals, and wage loss compensation applications. Each form serves a specific function in the workers' compensation process, making it essential to select the correct one for your needs.
Forms not included in the OS-24 are not available through the Bureau of Workers' Compensation. However, you can obtain Industrial Commission of Ohio forms by calling their forms and publications number at 614-644-8009. It is important to ensure you have the correct form for your specific situation to avoid delays in processing.