Fill a Valid Ohio Bwc Writable C 9 Form
Fill a Valid Ohio Bwc Writable C 9 Form
At What Age Do You Stop Paying Property Taxes in Ohio - Consists of specific fields to ensure all relevant information is gathered.
For businesses and employees alike, understanding the crucial aspects of a New York Non-compete Agreement form can significantly impact their legal standing and operational strategies moving forward.
Jfs Forms Central - Additional documentation may be requested if space is insufficient.
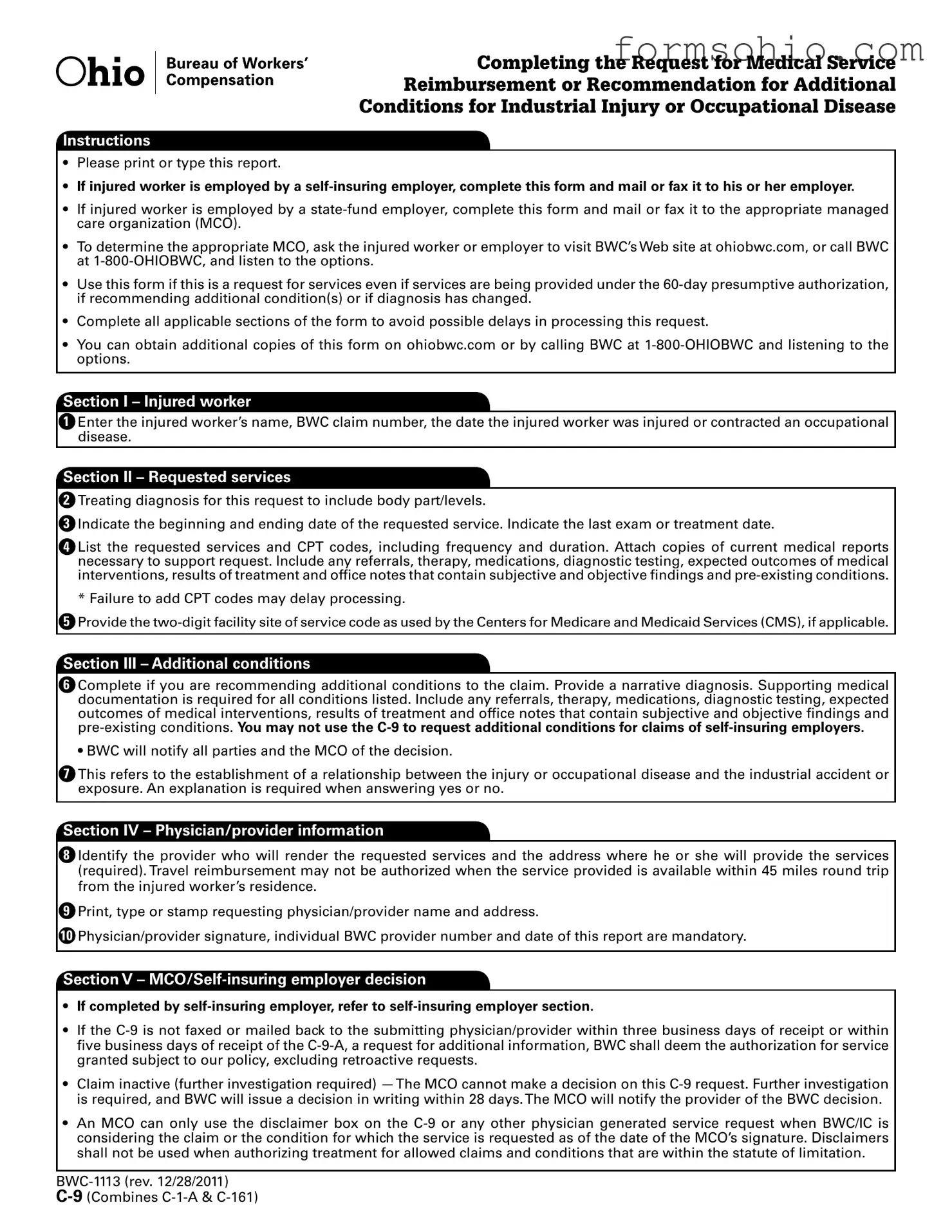
Completing the Request for Medical Service
Reimbursement or Recommendation for Additional
Conditions for Industrial Injury or Occupational Disease
Instructions
•Please print or type this report.
•If injured worker is employed by a
•If injured worker is employed by a
•To determine the appropriate MCO, ask the injured worker or employer to visit BWC’s Web site at ohiobwc.com, or call BWC at
•Use this form if this is a request for services even if services are being provided under the
•Complete all applicable sections of the form to avoid possible delays in processing this request.
•You can obtain additional copies of this form on ohiobwc.com or by calling BWC at
Section I – Injured worker
1Enter the injured worker’s name, BWC claim number, the date the injured worker was injured or contracted an occupational disease.
Section II – Requested services
2Treating diagnosis for this request to include body part/levels.
3Indicate the beginning and ending date of the requested service. Indicate the last exam or treatment date.
4List the requested services and CPT codes, including frequency and duration. Attach copies of current medical reports necessary to support request. Include any referrals, therapy, medications, diagnostic testing, expected outcomes of medical interventions, results of treatment and ofice notes that contain subjective and objective indings and
*Failure to add CPT codes may delay processing.
5Provide the
Section III – Additional conditions
6Complete if you are recommending additional conditions to the claim. Provide a narrative diagnosis. Supporting medical documentation is required for all conditions listed. Include any referrals, therapy, medications, diagnostic testing, expected outcomes of medical interventions, results of treatment and ofice notes that contain subjective and objective indings and
• BWC will notify all parties and the MCO of the decision.
7This refers to the establishment of a relationship between the injury or occupational disease and the industrial accident or exposure. An explanation is required when answering yes or no.
Section IV – Physician/provider information
8Identify the provider who will render the requested services and the address where he or she will provide the services (required). Travel reimbursement may not be authorized when the service provided is available within 45 miles round trip from the injured worker’s residence.
9Print, type or stamp requesting physician/provider name and address.
10Physician/provider signature, individual BWC provider number and date of this report are mandatory.
Section V –
•If completed by
•If the
•Claim inactive (further investigation required)
•An MCO can only use the disclaimer box on the
Request for Medical Service Reimbursement or Recommendation for Additional Conditions for Industrial Injury or Occupational Disease
• Instructions for completing the
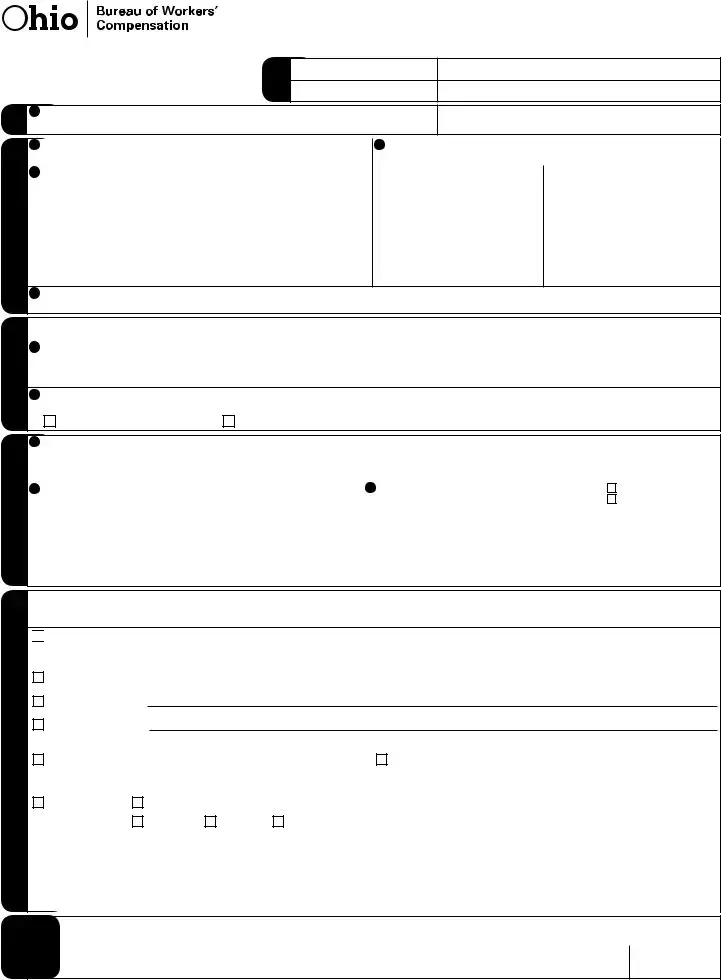
IW |
1 Injured worker name |
|
|
|
|
Fax note
To
From
|
Phone number |
|
|
Phone number |
|
Fax number |
|
Claim number |
|
Date of injury |
|
|
|
||
|
|
||
|
|
/ |
/ |
II. Requested services |
|
III. Additional conditions |
|
Physician/provider |
information |
IV. |
|
V.
2 |
Treating diagnosis for this request to include body part/levels. |
3 Date service begins |
Date service ends |
Date of last exam or treatment |
|||
|
|
/ |
/ |
/ |
/ |
/ |
/ |
4 |
Requested services with CPT/HCPCS codes (required) |
|
Frequency |
|
|
Duration |
|
1. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4. |
|
|
|
|
|
|
|
5Provide the
If you are recommending additional conditions to the claim, supporting documentation is required. You may not use the C9 to request
additional conditions for claims of
6Provide diagnosis (narrative description only), and location and site for conditions you are requesting.
7In your opinion, based on the history from the injured worker, your clinical evaluation and expertise, is the diagnosis or condition causally related, either directly or proximately, to the alleged industrial accident or exposure?
|
Yes, please attach explanation. |
|
No, please attach explanation. |
8Identify the provider who will render the requested services and the address where he or she will provide the services (required).Travel reimbursement may not be authorized when the service provided is available within 45 miles round trip from the injured worker’s residence.
9 |
Requesting physician/provider name and address (please print, type, or |
10 Physician/provider/authorized signature (required) |
POR |
|
stamp) |
|
Not POR — but treating |
|
|
|
physician/provider |
|
|
Individual BWC provider number (required) |
Date (M/D/Y) (required) |
|
|
|
|
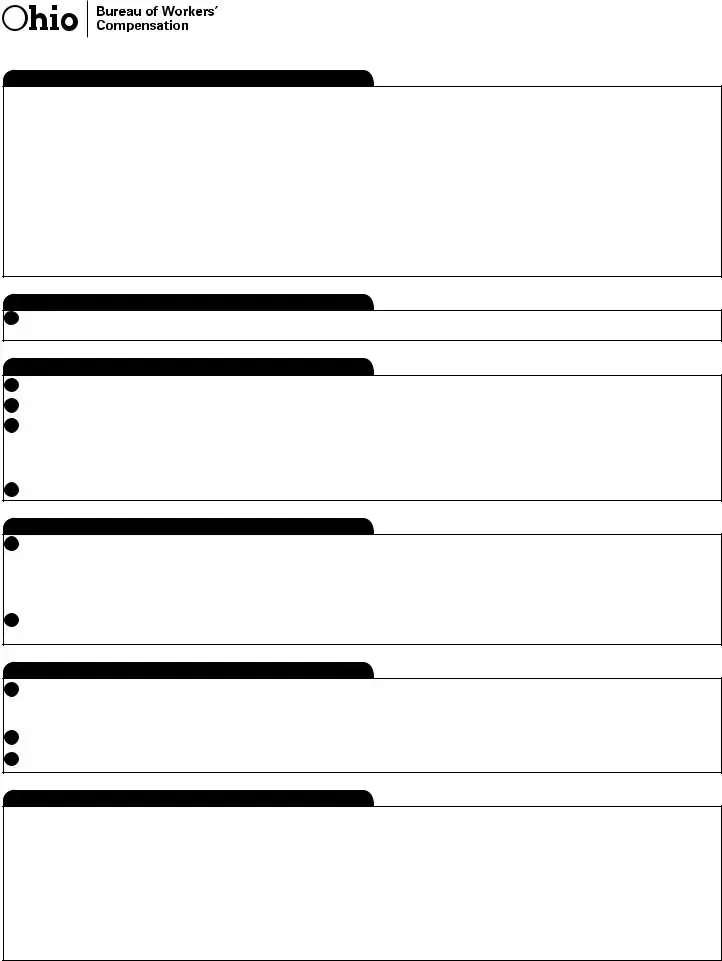
I certify the above information is correct to the best of my knowledge. I am aware that any person who knowingly makes a false statement, misrepresentation, concealment of fact or any other act of fraud to obtain payment as provided by BWC or who knowingly accepts payment to which that person is not entitled, is subject to felony criminal prosecution and may, under appropriate criminal provisions, be punished by a ine, imprisonment, or both.
Managed care organization (MCO) — If this page is not faxed or mailed back to the submitting physician/provider within three business days of receipt or within ive business days of receipt of information requested on the

 Approved with disclaimer — This medical payment authorization is based upon a claim or additional condition that BWC/IC is considering as of the date of the MCO’s signature. If the claim or additional condition is ultimately disallowed, BWC may not cover the services/supplies to which this medical payment authorization applies.These services/supplies may be the responsibility of the injured worker (for MCO use only).
Approved with disclaimer — This medical payment authorization is based upon a claim or additional condition that BWC/IC is considering as of the date of the MCO’s signature. If the claim or additional condition is ultimately disallowed, BWC may not cover the services/supplies to which this medical payment authorization applies.These services/supplies may be the responsibility of the injured worker (for MCO use only).
Approved |
Date service begins _____ /_____ /_____ |
Date service ends _____ /_____ /_____ |
Amended approval:
Denied explanation:
You may ile disputes to the decision in writing with supporting documentation to the MCO.
Pending: The documentation requested must be submitted to |
Claim inactive: MCO cannot make a decision on this request, |
||||||||
the MCO case manager within 10 business days to allow for a |
further investigation required. BWC will issue a decision in writing |
||||||||
treatment decision. Failure to respond may result in denial. |
within 28 days. |
|
|
|
|
||||
Withdrawn |
Dismissed |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
BWC claim status: |
Allowed |
Denied |
Pending |
|
|
|
|
|
|
MCO |
|
MCO name and signature (print, type or stamp and sign) |
|
|
|||||
(please print, type or stamp) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MCO number |
Telephone number |
Date |
|
|
|
|
|
|
|
|
|
( ) |
/ |
/ |
|
employer |
|||||
authorization for treatment shall be deemed granted, per Ohio Administrative Code |
/ |
/ |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Date |
|
|
|
|
|
|
|
|
| Fact Name | Fact Description |
|---|---|
| Form Purpose | The C-9 form is used to request medical service reimbursement or recommend additional conditions for industrial injuries or occupational diseases. |
| Governing Law | This form is governed by Ohio Administrative Code 4123-19-03. |
| Submission Process | If the injured worker has a self-insuring employer, the form must be sent to that employer. For state-fund employers, it should be sent to the appropriate managed care organization (MCO). |
| 60-Day Authorization | The form can be used even if services are being provided under the 60-day presumptive authorization. |
| Medical Documentation | All requested services must include current medical reports and supporting documentation to avoid delays. |
| CPT Codes Requirement | Failure to include CPT codes may result in processing delays for the request. |
| Provider Information | Physician/provider information, including name and address, is mandatory on the form. |
| Decision Notification | BWC will notify all parties and the MCO of the decision regarding the request. |
| Claim Inactive Status | If the claim is inactive, further investigation is required, and BWC will issue a decision within 28 days. |
| Disclaimers | Disclaimers on the C-9 can only be used when the claim is under consideration by BWC/IC. |
The Ohio BWC Writable C-9 form is an essential document for requesting medical service reimbursement or recommending additional conditions related to industrial injuries or occupational diseases. Along with this form, several other documents are often required to ensure a smooth processing experience. Below is a list of these documents, each accompanied by a brief description.
Each of these documents plays a significant role in ensuring that the injured worker receives the necessary medical care and compensation. Proper completion and submission of these forms can help avoid delays and facilitate a smoother claims process.
Filling out the Ohio BWC Writable C-9 form is a crucial step for obtaining medical service reimbursement or recommending additional conditions related to an industrial injury or occupational disease. Following the instructions carefully will help ensure that the request is processed smoothly and efficiently.
Completing the Ohio BWC Writable C-9 form can be a challenging task, and many individuals make common mistakes that can delay the processing of their requests. One frequent error is not completing all applicable sections of the form. Each section is designed to gather essential information, and leaving any part blank can lead to significant delays. It is crucial to ensure that every section is filled out thoroughly to avoid unnecessary holdups in processing.
Another mistake often seen is the omission of necessary documentation. The form requires supporting medical reports, including referrals, therapy details, and diagnostic testing results. Failing to attach these documents can result in the request being denied or delayed. Always double-check that all required documents are included before submission.
Many people also overlook the importance of including CPT codes. These codes are vital for identifying the specific services being requested. Without them, processing can be stalled, as the reviewing party may not understand the nature of the requested services. It is advisable to verify that all CPT codes are accurately listed to ensure a smooth review process.
In addition, some individuals do not provide a clear narrative diagnosis when recommending additional conditions. The form specifically asks for a detailed explanation of the conditions being requested. A vague or incomplete description can lead to confusion and may result in a denial of the request. Providing a well-defined narrative can significantly enhance the chances of approval.
Another common oversight involves the physician/provider information section. It is mandatory to include the provider’s name, address, and signature. Incomplete or inaccurate information can lead to processing delays. Ensuring that this section is filled out correctly is essential for the timely approval of services.
Lastly, individuals sometimes fail to understand the importance of timely submission. If the C-9 form is not returned within the specified timeframe, the authorization for services may be automatically granted. However, this can lead to complications if the claim is later disallowed. Keeping track of submission deadlines and following up as needed can help prevent these issues.
What is the Ohio BWC Writable C-9 form?
The Ohio BWC Writable C-9 form is a request for medical service reimbursement or a recommendation for additional conditions related to an industrial injury or occupational disease. This form is essential for injured workers seeking medical services covered under Ohio's workers' compensation system.
Who should complete the C-9 form?
The form should be completed by the treating physician or provider of the injured worker. If the worker is employed by a self-insuring employer, the completed form must be sent directly to that employer. For those working with a state-fund employer, it should be sent to the appropriate managed care organization (MCO).
How do I find the appropriate MCO for the injured worker?
You can find the appropriate MCO by visiting the Ohio Bureau of Workers' Compensation (BWC) website at ohiobwc.com or by calling BWC at 1-800-OHIOBWC. They provide options to help you identify the right MCO.
What information is required in Section I of the C-9 form?
In Section I, you need to provide the injured worker's name, BWC claim number, and the date of the injury or the onset of the occupational disease. This information is crucial for processing the request accurately.
What details must be included in Section II regarding requested services?
Section II requires you to list the treating diagnosis, the start and end dates for the requested services, and the date of the last exam or treatment. You also need to include the requested services along with their CPT codes, frequency, and duration. Attach any relevant medical reports that support your request.
Can I request additional conditions using the C-9 form?
You can request additional conditions, but only if the worker is not employed by a self-insuring employer. You must provide a narrative diagnosis and supporting medical documentation for all additional conditions listed. This ensures that the request is thorough and complete.
What happens if the C-9 form is not processed within the specified time frame?
If the form is not faxed or mailed back to the submitting physician/provider within three business days, or within five days of receiving a request for additional information, the authorization for service will be deemed granted, subject to BWC policies. This excludes retroactive requests.
What should I include in the physician/provider information section?
In this section, you must identify the provider who will render the requested services and provide their address. It’s also important to include the physician's name, BWC provider number, and signature. This information is mandatory for processing the request.
What if the claim is inactive or further investigation is required?
If the claim is inactive, the MCO cannot make a decision on the C-9 request. Further investigation will be needed, and BWC will issue a decision in writing within 28 days. The MCO will notify the provider of the outcome.
How can I obtain additional copies of the C-9 form?
Additional copies of the C-9 form can be obtained from the BWC website at ohiobwc.com or by calling BWC at 1-800-OHIOBWC. They will provide you with the necessary forms and guidance.