Fill a Valid Ohio Behavioral Discharge Form
Fill a Valid Ohio Behavioral Discharge Form
Soqic Ohio - The initiative emphasizes the importance of client feedback in treatment.
A Georgia Quitclaim Deed form is a legal document used to transfer ownership of property in Georgia with no guarantee about the clearness of the title. This type of deed simply transfers whatever interest the seller has in the property, if any, to the buyer. It's commonly used among family members or to clear up title issues, and you can find more information on this process at smarttemplates.net.
Ohio Drug Free Workplace - Addressing potential hazards using the form can prevent accidents and improve workplace morale.
|
Ohio Behavioral Health |
|
|
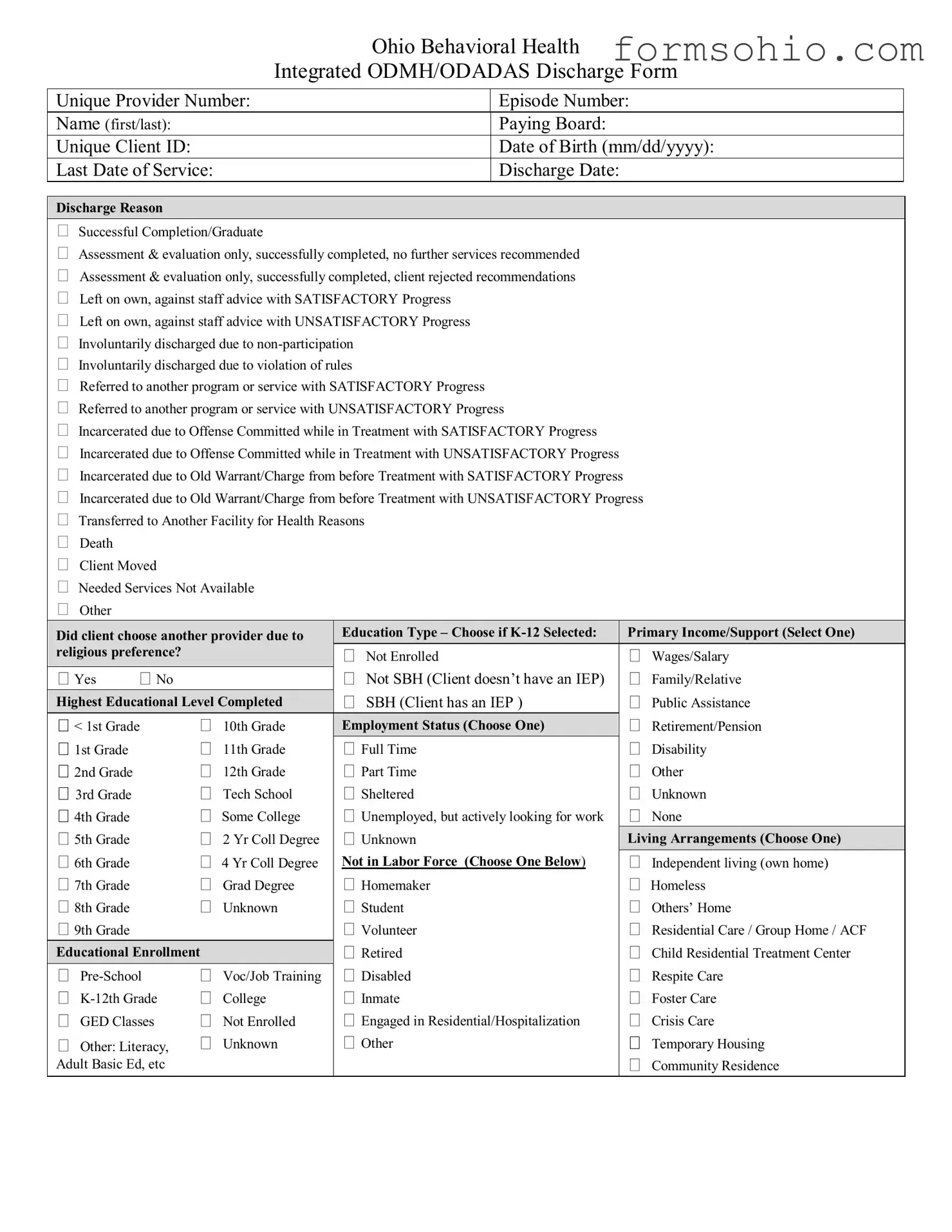
Integrated ODMH/ODADAS Discharge Form |
|
|
|
|
Unique Provider Number: |
|
Episode Number: |
Name (first/last): |
|
Paying Board: |
Unique Client ID: |
|
Date of Birth (mm/dd/yyyy): |
Last Date of Service: |
|
Discharge Date: |
 Discharge Reason
Discharge Reason
Successful Completion/Graduate
Assessment & evaluation only, successfully completed, no further services recommended
Assessment & evaluation only, successfully completed, client rejected recommendations
Left on own, against staff advice with SATISFACTORY Progress
Left on own, against staff advice with UNSATISFACTORY Progress
Involuntarily discharged due to
Involuntarily discharged due to violation of rules
Referred to another program or service with SATISFACTORY Progress
Referred to another program or service with UNSATISFACTORY Progress
Incarcerated due to Offense Committed while in Treatment with SATISFACTORY Progress
Incarcerated due to Offense Committed while in Treatment with UNSATISFACTORY Progress
Incarcerated due to Old Warrant/Charge from before Treatment with SATISFACTORY Progress
Incarcerated due to Old Warrant/Charge from before Treatment with UNSATISFACTORY Progress
Transferred to Another Facility for Health Reasons
Death
Client Moved
Needed Services Not Available
Other
|
|
|
|
|
|
Education Type – Choose if |
|
|
Primary Income/Support (Select One) |
|
|
|
|
|
|
|
|
|
|
||
|
|
|
||||||||
|
Did client choose another provider due to |
|
||||||||
|
religious preference? |
|
|
|
Not Enrolled |
|
Wages/Salary |
|||
|
|
|
|
|
|
|
||||
|
Yes |
No |
|
|
|
Not SBH (Client doesn’t have an IEP) |
|
Family/Relative |
||
|
Highest Educational Level Completed |
|
|
SBH (Client has an IEP ) |
|
Public Assistance |
||||
|
|
|
|
|||||||
|
< 1st Grade |
|
10th Grade |
|
Employment Status (Choose One) |
|
|
Retirement/Pension |
||
|
1st Grade |
|
11th Grade |
|
Full Time |
|
Disability |
|||
|
2nd Grade |
|
12th Grade |
|
Part Time |
|
Other |
|||
|
3rd Grade |
|
Tech School |
|
Sheltered |
|
Unknown |
|||
|
4th Grade |
|
Some College |
|
Unemployed, but actively looking for work |
|
None |
|||
|
5th Grade |
|
2 Yr Coll Degree |
|
Unknown |
|
Living Arrangements (Choose One) |
|
||
|
6th Grade |
|
4 Yr Coll Degree |
|
Not in Labor Force (Choose One Below) |
|
Independent living (own home) |
|||
|
7th Grade |
|
Grad Degree |
|
Homemaker |
|
Homeless |
|||
|
8th Grade |
|
Unknown |
|
Student |
|
Others’ Home |
|||
|
9th Grade |
|
|
|
|
Volunteer |
|
Residential Care / Group Home / ACF |
||
|
|
|
|
Retired |
|
Child Residential Treatment Center |
||||
|
Educational Enrollment |
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
Voc/Job Training |
|
Disabled |
|
Respite Care |
||||
|
College |
|
Inmate |
|
Foster Care |
|||||
|
GED Classes |
|
Not Enrolled |
|
Engaged in Residential/Hospitalization |
|
Crisis Care |
|||
|
Other: Literacy, |
Unknown |
|
Other |
|
Temporary Housing |
||||
Adult Basic Ed, etc |
|
|
|
|
|
|
Community Residence |
|||
|
|
|
|
|
|
|
|
|
|
|
|
Living Arrangements (continued) |
|
|
Drug of Choice (Continued) |
|
|
ODMH: BIOMARKERS |
|
|||||||
|
|
|
|
|
|
||||||||||
|
Nursing Facility |
|
|
|
|
|
|
|
|||||||
|
|
|
|
Source of Height/Weight Information |
|
||||||||||
|
Licensed MR Facility |
|
|
Other Opiates and Synthetics |
|
||||||||||
|
State MH/MR Institution |
|
|
PCP |
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|||||
|
Hospital |
|
|
|
Other Hallucinogens |
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
Height and Weight |
|
|||||||
|
Correctional Facility |
|
|
Methamphetamines |
|
|
|
|
|
Height (feet and inches) |
|||||
|
Other |
|
|
|
Other Amphetamines |
|
|
| |
|
||||||
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|||||||
|
Unknown |
|
|
Other Stimulants |
|
|
|
|
|
Weight (lbs) |
|||||
|
|
|
|
|
|
Benzodiazepines |
|
|
| |
|
|||||
|
|
|
Global Assessment of |
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
||||||
| |
|
Functioning |
|
|
Other |
|
Physical Health Conditions |
|
|||||||
|
Diagnosis Type (Choose One) |
|
|
Barbiturates |
|
|
|
Does client report/provide evidence of any of the |
|||||||
|
DSM IV |
ICD9 |
|
|
Other |
|
following conditions in past year? |
||||||||
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
Diabetes |
|
|
|||||
|
Primary Diagnosis Code: |
|
|
Inhalants |
|
|
|
|
|
||||||
|
|
|
|
|
|
|
High Cholesterol |
||||||||
|
|
|
|
|
|
Nicotine |
|
|
|
|
Cardiovascular Disease (heart attack, stroke) |
||||
|
Secondary Diagnosis Code: |
|
|
Other Medications |
|
|
|
High blood pressure |
|||||||
|
|
|
|
|
|
Unknown |
|
|
|
Cancer |
|
|
|||
|
|
|
|
|
|
Frequency of Use |
|
|
|
Kidney Disease/Failure |
|||||
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
– 3 X Past Week |
|
Bowel Obstruction (eg, constipation) |
|||||||
|
Tertiary Diagnosis Code: |
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
– 2 X in Past Mo |
– 6 X Past Week |
|
Respiratory Disease (eg, COPD) |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
None |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
Special Populations (Select all that Apply) |
|
|
Route of Administration |
|
|
|
Health Care Utilization |
|
||||||
|
SMD/SED |
|
|
Oral |
|
Injection |
|
How frequently (in days) has the client used the |
|||||||
|
Alcohol/Other Drug Abuse |
|
|
Smoking |
|
Other |
|
following since admission or last update? |
|||||||
|
|
|
|
|
|
|
|
|
|||||||
|
Forensic Status |
|
|
Inhalation |
Unknown |
|
|
|
|
|
|||||
|
|
|
|
|
|
Hospital Admissions |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
| |
|
|||
|
Developmentally Disabled |
|
|
|
|
Age of First Use – First |
|
||||||||
|
|
|
|
|
|
|
|
||||||||
|
Deaf/Hard of Hearing |
|
| |
|
Intoxication |
|
|
|
|
|
Emergency Room Visits/Admits |
||||
|
|
|
|
|
|
|
|
|
|||||||
|
Blind/Sight Impaired |
|
|
Primary AOD Code: |
|
|
| |
|
(psychiatric or physical health) |
||||||
|
|
|
|
|
|
|
|
||||||||
|
Physically Disabled |
|
|
|
|
Number of Arrests past 30 days |
|
|
|
Outpatient Primary Care Visits |
|||||
|
Sexual Abuse Victim |
|
| |
|
(AOD NOM) |
| |
|
(physical health) |
|||||||
|
Domestic Violence Victim/Witness |
|
|
Primary Reimbursement (Select One) |
|
|
|
|
Dental Visits |
||||||
|
Child of Alcohol/Drug Abuser |
|
|
|
|
|
|
| |
|
||||||
|
|
|
|
|
|
|
|
|
|||||||
|
HIV/AIDS |
|
|
Blue Cross/Blue Shield |
|
|
|
Evidence Based Practices |
|
||||||
|
Suicidal |
|
|
|
Medicare |
|
|
|
|
Did the client receive any of the following EBPs |
|||||
|
Language Barriers/English 2ND Lang. |
|
|
Medicaid |
|
|
|
|
since admission or last update? |
||||||
|
Hepatitis C |
|
|
Other Government Support |
|
Adult Practices |
|
||||||||
|
Transgendered |
|
|
Worker’s Compensation |
|
Supportive Housing |
|||||||||
|
In Custody/Child Welfare |
|
|
Other Private Health Insurance |
|
Supported Employment |
|||||||||
|
Multiple Service System Involvement |
|
|
No Charge |
|
|
|
Assertive Community Treatment (ACT) |
|||||||
|
|
|
|
Other Payment Source |
|
|
|
|
|
||||||
|
Early Childhood: At Risk for SED |
|
|
|
|
|
Family |
|
|||||||
|
Sexual Offender |
|
|
|
|
IDDT |
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
Frequency of attendance at |
|
|
|
|
||||||||
|
Bisexual/Gay/Lesbian |
|
|
programs in the 30 days prior to discharge |
|
|
WMR/Illness |
||||||||
|
|
|
|
|
|
|
|
|
|||||||
|
Military Family |
|
|
No attendance in past month |
|
Medication Management |
|||||||||
|
Drug of Choice (Primary Choice) |
|
|
|
Child & Adolescent Practices |
|
|||||||||
|
Alcohol |
|
|
|
|
Therapeutic Foster Care |
|||||||||
|
Cocaine/Crack |
|
|
Some but unknown |
Unknown |
|
|
||||||||
|
|
|
|
|
|
Functional Family Therapy |
|||||||||
|
Marijuana/Hashish |
|
|
Does the client use tobacco products? |
|
|
|||||||||
|
Heroin |
|
|
|
Yes |
No |
Don’t Know |
|
Intensive |
||||||
|
Drug of Choice (Secondary) |
|
|
Drug of Choice (Tertiary) |
|
|
||||
|
|
|
|
|
||||||
|
Alcohol |
|
|
|
Alcohol |
|
|
|
||
|
Cocaine/Crack |
|
|
Cocaine/Crack |
|
|||||
|
Marijuana/Hashish |
|
|
Marijuana/Hashish |
|
|||||
|
Heroin |
|
|
|
Heroin |
|
|
|
||
|
|
|||||||||
|
Other Opiates and Synthetics |
|
Other Opiates and Synthetics |
|||||||
|
PCP |
|
|
|
PCP |
|
|
|
||
|
Other Hallucinogens |
|
|
Other Hallucinogens |
|
|||||
|
Methamphetamines |
|
|
Methamphetamines |
|
|||||
|
Other Amphetamines |
|
|
Other Amphetamines |
|
|||||
|
Other Stimulants |
|
|
Other Stimulants |
|
|||||
|
Benzodiazepines |
|
|
Benzodiazepines |
|
|||||
|
Other |
|
Other |
|||||||
|
Barbiturates |
|
|
Barbiturates |
|
|||||
|
Other |
|
Other |
|||||||
|
Inhalants |
|
|
|
Inhalants |
|
|
|
||
|
|
|||||||||
|
Nicotine |
|
|
|
Nicotine |
|
|
|
||
|
Other Medications |
|
|
Other Medications |
|
|||||
|
Unknown |
|
|
Unknown |
|
|||||
|
None |
|
|
|
None |
|
|
|
||
Frequency of Use |
|
Frequency of Use |
|
|||||||
|
No use Past Mo |
1 – 3 X Past Week |
|
No use Past Mo |
1 – 3 X Past Week |
|||||
|
1 – 2 X in Past Mo |
3 – 6 X Past Week |
|
1 – 2 X in Past Mo |
3 – 6 X Past Week |
|||||
|
Daily |
|
Unknown |
|
Daily |
|
|
Unknown |
||
Route of Administration |
|
Route of Administration |
|
|||||||
|
Oral |
|
Injection |
|
Oral |
|
|
Injection |
||
|
Smoking |
|
Other |
|
Smoking |
|
|
Other |
||
|
Inhalation |
|
Unknown |
|
Inhalation |
|
|
Unknown |
||
|
|
|
|
|
|
|
|
|||
|
|
|
Age of First Use – First |
|
|
|
Age of First Use – First |
|||
| |
|
Intoxication |
|
| |
|
Intoxication |
|
|||
|
|
|
|
|
|
|
||||
|
Secondary AOD Code |
|
|
Tertiary AOD Code |
|
|||||
|
|
|
|
|
|
|
|
|
|
|
| Fact Name | Details |
|---|---|
| Form Title | Ohio Behavioral Health Integrated ODMH/ODADAS Discharge Form |
| Governing Laws | Ohio Revised Code Sections 5119.22 and 5119.23 |
| Provider Information | Includes Unique Provider Number and Episode Number. |
| Client Identification | Requires Name, Unique Client ID, and Date of Birth. |
| Discharge Reasons | Multiple options, including Successful Completion and Involuntary Discharge. |
| Living Arrangements | Options include Independent Living, Homeless, and Residential Care. |
| Health Conditions | Captures physical health conditions and associated diagnosis codes. |
| Substance Use Information | Records primary and secondary drug of choice, frequency of use. |
| Evidence-Based Practices | Documents any EBPs received since admission or last update. |
The Ohio Behavioral Discharge form is a crucial document used in the discharge process for individuals receiving behavioral health services. Alongside this form, several other documents are commonly utilized to ensure a comprehensive understanding of the client's treatment and ongoing needs. Below is a list of five such documents, each serving a specific purpose in the discharge process.
Each of these documents plays a vital role in ensuring that clients receive appropriate care and support after their discharge from behavioral health services. Proper documentation and communication are key to facilitating a smooth transition for clients as they move forward in their recovery journey.
Once you have gathered all necessary information, you can begin filling out the Ohio Behavioral Discharge form. This form is essential for documenting the details of a client's discharge from behavioral health services. Ensure that you have all relevant information on hand to complete each section accurately.
Filling out the Ohio Behavioral Discharge form can be straightforward, but many people make common mistakes that can lead to complications. One frequent error is failing to provide accurate personal information. This includes the client’s name, date of birth, and unique client ID. If these details are incorrect, it may cause delays in processing and can affect the client's access to future services. Always double-check this information before submitting the form.
Another mistake is neglecting to select the appropriate discharge reason. The form includes various options, such as “Successful Completion” or “Involuntarily discharged due to non-participation.” Choosing the wrong reason can lead to misunderstandings about the client's status and needs. It’s essential to select the option that best reflects the client’s situation to ensure they receive the appropriate follow-up care.
People often overlook the section regarding the client’s educational background and employment status. This information is vital for understanding the client’s support system and can influence future treatment plans. Missing or incorrect entries in these sections can lead to gaps in care. Make sure to provide complete and accurate details about the client’s education and employment situation.
Lastly, individuals sometimes skip over the health conditions and medication sections. These areas are crucial for a comprehensive understanding of the client’s physical and mental health. Failing to report existing health issues or current medications can hinder effective treatment. It’s important to provide as much detail as possible in these sections to ensure the client receives the best care moving forward.
What is the purpose of the Ohio Behavioral Discharge form?
The Ohio Behavioral Discharge form is designed to document the discharge of clients from behavioral health services. It captures essential information about the client's treatment episode, including the reason for discharge, client demographics, and any relevant health conditions. This information is vital for ensuring continuity of care and for reporting purposes.
What information is required on the form?
The form requires several pieces of information, including:
Additional details regarding the client's educational background, employment status, living arrangements, and health conditions may also be required.
What are the discharge reasons listed on the form?
The form includes various discharge reasons, such as:
Each reason provides insight into the client's journey and outcomes during treatment.
How does the form handle client confidentiality?
The Ohio Behavioral Discharge form is subject to confidentiality regulations. Personal information must be handled with care to protect the client's privacy. Only authorized personnel should have access to the completed forms, and they should be stored securely in compliance with applicable laws.
Can the form be used for clients with special populations?
Yes, the form accommodates clients from special populations. It includes sections to identify clients who may be developmentally disabled, deaf or hard of hearing, victims of domestic violence, and more. This information is crucial for tailoring future services to meet their unique needs.
What happens if a client is involuntarily discharged?
If a client is involuntarily discharged, it is important to document the reason clearly on the form. This may include non-participation or violation of rules. The discharge process should follow established protocols to ensure the client is informed and that any necessary referrals are made.
Is there a specific process for submitting the form?
After completing the Ohio Behavioral Discharge form, it should be submitted according to the provider's established procedures. This may involve sending the form to a designated office or entering the information into a digital system. Ensuring timely submission is important for accurate record-keeping and continuity of care.